How Prolotherapy Helps in Treating Rotator Cuff Injuries
- Published on: 19/Feb/2026
- Posted By: Arka Health

Understanding Chronic Shoulder Pain Beyond Inflammation
Chronic shoulder pain is often misunderstood. Many patients are told they have “tendon inflammation” and are prescribed rest, anti inflammatory medication, or steroid injections. However, long standing rotator cuff problems are rarely pure inflammatory conditions. They are more accurately described as degenerative tendon disorders involving collagen disorganization, failed healing, and mechanical instability.
This shift in understanding has changed how clinicians approach treatment. Instead of suppressing inflammation, modern regenerative strategies focus on restoring tendon structure and joint stability. Prolotherapy for rotator cuff injuries works within this biological framework by stimulating collagen repair and strengthening the tendon attachment to bone.
For patients searching for non surgical shoulder repair, this approach offers a pathway that addresses root causes rather than temporarily masking pain.
Rotator Cuff Anatomy and Why It Fails
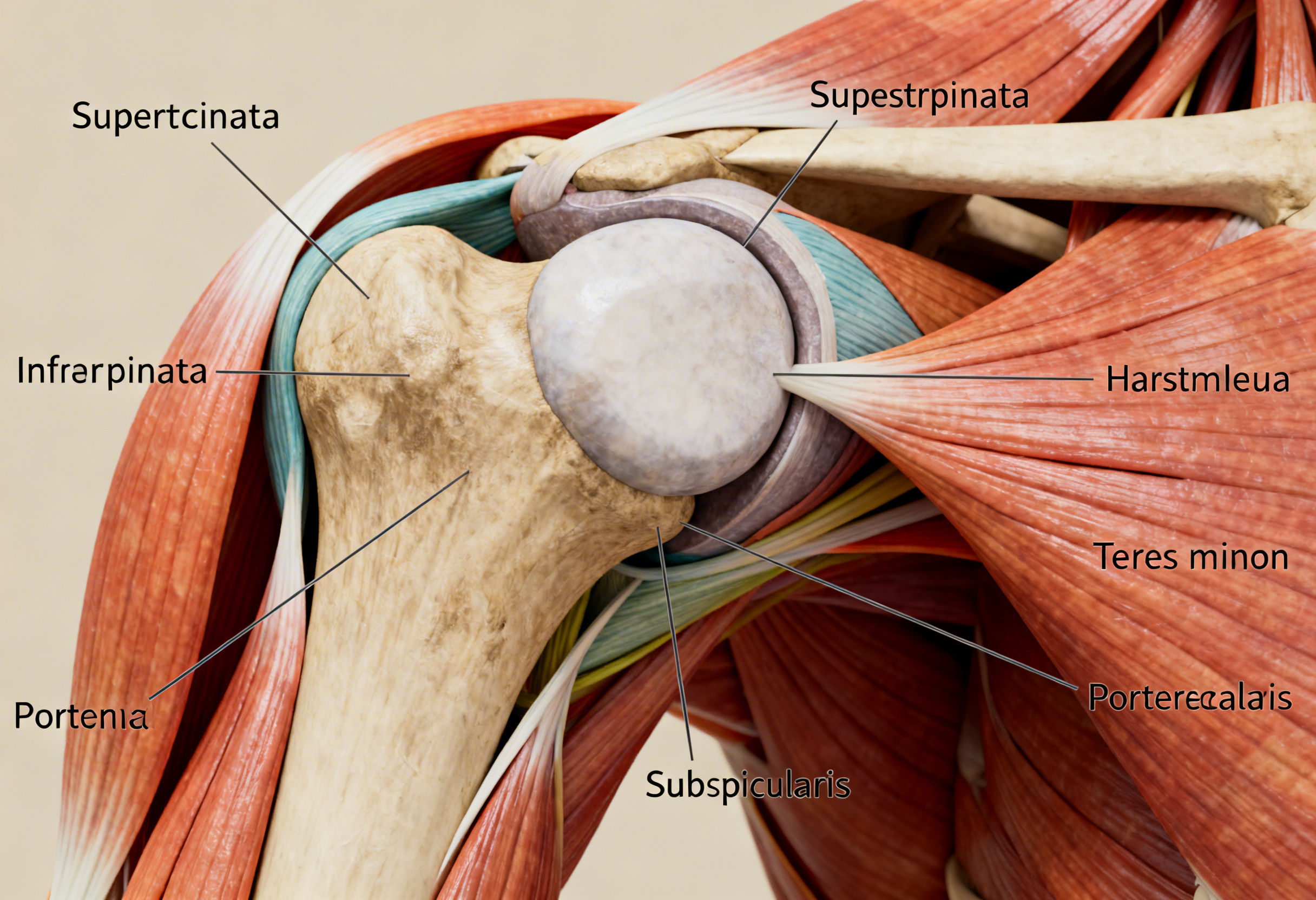
The rotator cuff consists of four muscles and their tendons:
- Supraspinatus
- Infraspinatus
- Teres minor
- Subscapularis
Together, these structures form a stabilizing hood around the humeral head. Their primary role is to maintain centralization of the ball within the glenoid socket during arm movement.
The supraspinatus tendon is the most frequently injured component. It contains a region called the critical zone, an area with relatively poor blood supply. Reduced vascularity limits the ability of tenocytes to repair micro damage. Over time, repetitive strain, metabolic stress, or mechanical impingement leads to collagen fiber breakdown.
Instead of healthy parallel Type I collagen, the tendon begins to accumulate weaker Type III collagen. This structural deterioration forms the basis of tendinosis.
From Tendinitis to Tendinosis to Tear
Rotator cuff pathology progresses along a continuum.
Tendinitis
An acute inflammatory response after sudden overload.
Tendinosis
A chronic degenerative state characterized by:
- Collagen disorganization
- Tenocyte apoptosis
- Increased non functional neovascularization
- Minimal inflammatory cells
Partial Thickness Tear
Focal structural disruption while still attached to bone.
Full Thickness Tear
Complete tendon separation from the humerus.
Prolotherapy for rotator cuff injuries is most effective during tendinosis and partial thickness tear stages. At this point, biological repair potential still exists.
Why Conventional Treatments Often Fail
Steroid Injections
Corticosteroids reduce pain quickly. However, research shows they:
- Suppress collagen synthesis
- Increase tendon atrophy
- Reduce biomechanical strength
- Increase risk of rupture with repeated use
Steroids address symptoms but may worsen structural integrity.
NSAIDs
Non steroidal anti inflammatory drugs inhibit prostaglandin pathways necessary for tissue repair. Chronic use interferes with tendon remodeling.
Passive Physiotherapy Alone
While rehabilitation is essential, exercise alone cannot reverse advanced collagen degeneration without biological stimulation.
This creates a treatment gap for patients seeking shoulder injury repair without surgery.
How Prolotherapy Works Biologically
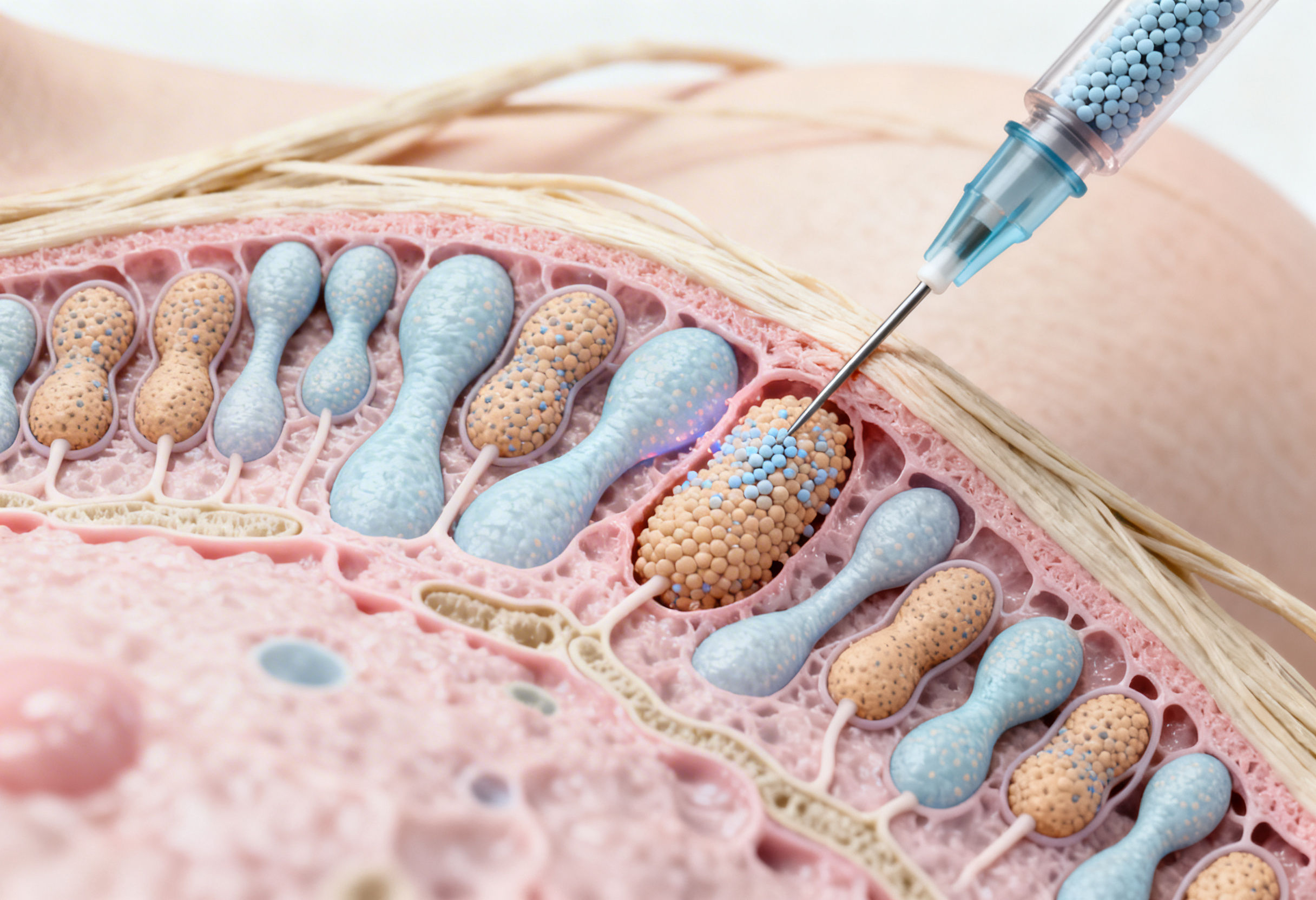
Prolotherapy involves injecting hypertonic dextrose solution into damaged tendon and ligament attachments.
Step 1: Controlled Local Inflammatory Trigger
The concentrated dextrose creates osmotic stress, activating local cellular signaling pathways. This stimulates the release of growth factors such as:
- Transforming Growth Factor beta
- Platelet Derived Growth Factor
- Insulin like Growth Factor
This is not harmful inflammation. It is a targeted regenerative stimulus.
Step 2: Fibroblast Activation
Fibroblasts migrate to the injection site and begin synthesizing new collagen matrix.
The healing cascade moves through three phases:
- Inflammatory phase
- Proliferative phase
- Remodeling phase
Over weeks to months, immature Type III collagen is gradually replaced with stronger Type I collagen.
This increases tendon thickness, tensile strength, and resistance to further tearing.
Step 3: Ligament Stabilization
Shoulder instability contributes significantly to rotator cuff overload. Prolotherapy for rotator cuff injuries strengthens supporting capsular ligaments, reducing excessive humeral head translation.
Improved stability decreases repetitive impingement and mechanical strain.
Step 4: Neurogenic Pain Modulation
Chronic shoulder pain often involves neurogenic inflammation mediated by Substance P and CGRP. Dextrose has been shown to influence TRPV1 receptor pathways, reducing peripheral nerve sensitization.
This explains why patients often report reduction in neuropathic shoulder pain alongside structural improvement.
The Role of Metabolic Health in Tendon Recovery
Tendon healing does not occur in isolation. Systemic metabolic factors strongly influence outcomes.
Insulin Resistance
Elevated glucose leads to Advanced Glycation End products that cross link collagen fibers, making them stiff and brittle.
Chronic Inflammation
Metabolic syndrome increases IL 6 and TNF alpha levels, inhibiting fibroblast function.
Obesity
Adipokines impair microvascular circulation, delaying tissue repair.
Optimizing metabolic health enhances response to prolotherapy for rotator cuff injuries.
The Gut Joint Axis
Emerging evidence highlights the gut microbiome’s role in musculoskeletal health.
Gut dysbiosis increases intestinal permeability, allowing endotoxins into circulation. This promotes chronic low grade inflammation that interferes with tendon remodeling.
Addressing gut health improves systemic inflammatory balance and supports regenerative outcomes.
Nutritional Support for Collagen Repair
Successful tendon regeneration requires biochemical substrates.
Key nutrients include:
- Vitamin C for collagen hydroxylation
- Proline and glycine for collagen backbone
- Zinc and copper for cross linking enzymes
- Omega 3 fatty acids for controlled inflammatory modulation
Without adequate nutritional support, regenerative therapies cannot achieve optimal structural outcomes.
Diagnostic Precision and Ultrasound Guidance

Static MRI imaging may detect tears but does not always correlate with pain. Many asymptomatic individuals show rotator cuff abnormalities.
Dynamic musculoskeletal ultrasound allows:
- Real time visualization during movement
- Detection of impingement
- Assessment of instability
- Accurate needle placement
Ultrasound guided prolotherapy improves precision and clinical outcomes.
What to Expect During Treatment
A typical prolotherapy session lasts 30 to 60 minutes.
After local anesthetic administration, dextrose solution is injected into:
- Tendon insertion points
- Capsular ligaments
- Areas of focal degeneration
Post procedure course:
Days 1 to 5
Mild soreness and stiffness, indicating inflammatory activation.
Weeks 2 to 4
Collagen deposition begins.
Months 2 to 6
Remodeling and strengthening phase.
Most patients require 3 to 6 sessions spaced several weeks apart.
Consistency is essential because collagen maturation is cumulative.

Who Is a Suitable Candidate
- Chronic rotator cuff tendinosis
- Partial thickness tears
- Shoulder instability
- Recurrent impingement
- Patients seeking non surgical shoulder repair
Massive retracted tears may require surgical evaluation.
ARKA Anugraha Hospital Approach
At ARKA Anugraha Hospital, prolotherapy for rotator cuff injuries is delivered within a systems based regenerative framework. Each patient undergoes structural assessment, metabolic screening, and functional evaluation before therapy planning. Dr Gaurang Ramesh integrates regenerative injections with targeted rehabilitation, nutritional optimization, and correction of biomechanical imbalances. The focus is long term tendon integrity and restoration of shoulder biomechanics rather than short term symptom suppression.
Conclusion
Chronic rotator cuff injuries are not merely inflammatory conditions. They represent structural degeneration influenced by mechanical stress, metabolic dysfunction, and impaired collagen remodeling.
Prolotherapy for rotator cuff injuries offers a biologically rational method to stimulate tendon repair, restore ligament stability, and improve shoulder function without surgery. When combined with metabolic correction and rehabilitation, it provides a comprehensive path toward durable recovery.
FREQUENTLY ASKED QUESTIONS
- How many prolotherapy sessions are needed for rotator cuff injuries?
Most patients require 3 to 6 sessions depending on severity. - Is prolotherapy painful?
Mild discomfort occurs during injection but is usually well tolerated. - How soon will I see improvement?
Improvement typically begins within 6 to 12 weeks. - Can prolotherapy heal partial tears?
Yes, partial thickness tears respond well due to preserved attachment. - Is it better than steroid injections?
Steroids suppress inflammation. Prolotherapy stimulates repair. - Can I exercise after treatment?
Light movement is encouraged. Heavy lifting is avoided initially. - Does prolotherapy rebuild collagen?
Yes, it stimulates fibroblast driven collagen synthesis. - Is ultrasound guidance necessary?
It significantly improves precision and outcomes. - Is prolotherapy safe for diabetics?
Yes, but glucose control improves healing response. - Does it treat shoulder instability?
Yes, it strengthens capsular ligaments. - Can it prevent surgery?
In many moderate cases, yes. - Are there side effects?
Temporary soreness and bruising are common. - Is nutritional support important?
Yes, collagen synthesis depends on adequate nutrients. - How long does recovery take?
Collagen remodeling continues for several months. - Is this part of regenerative medicine?
Yes, prolotherapy is a core regenerative therapy.
Explore Arka Recipes
Discover recipes that blend taste with health, crafted by our experts for your well-being.

Arka Diagnostics
Discover groundbreaking diagnostic services exclusive to India, now available at Arka Health, Bangalore