Prolotherapy for Lower Back Pain: Restoring Stability to Your Spine
- Published on: 18/Feb/2026
- Posted By: Arka Health

Chronic lower back pain is no longer a niche complaint. It is a global, growing health burden. Current estimates suggest low back pain affected ~619 million people worldwide in 2020, with projections rising to ~843 million by 2050. (ScienceDirect) For many patients, pain between the rib margin and the gluteal folds becomes persistent, recurrent, and resistant to “standard care” cycles of painkillers, rest, and occasional injections.
What often gets missed is a simple biomechanical truth: many chronic lower back pain patterns are driven by instability, not just “tight muscles” or “a disc issue.” When spinal ligaments lose tension after repetitive microtrauma, pregnancy-related laxity, sedentary deconditioning, injury, or degenerative change, the spine can develop abnormal segmental motion. That micro-motion repeatedly irritates pain-sensitive structures, such as facet joint capsules, periosteum, and ligament attachments, and the body compensates with chronic muscle guarding.
Prolotherapy for lower back pain (most commonly dextrose prolotherapy) is a regenerative injection approach designed to stimulate ligament repair, improve passive stability, and reduce pain driven by mechanical laxity. Systematic reviews describe prolotherapy as a regenerative intervention used for chronic low back pain, with outcomes that vary by patient selection, technique, diagnosis, and co-interventions. (MDPI)
At ARKA Anugraha Hospital, prolotherapy is positioned within an integrative, systems-based model: we treat the mechanical driver (instability) while also upgrading the internal terrain that determines tissue repair quality (metabolic health, inflammation, sleep, nutrition, and gut health).
The Stability Problem Most Back Pain Plans Do Not Solve

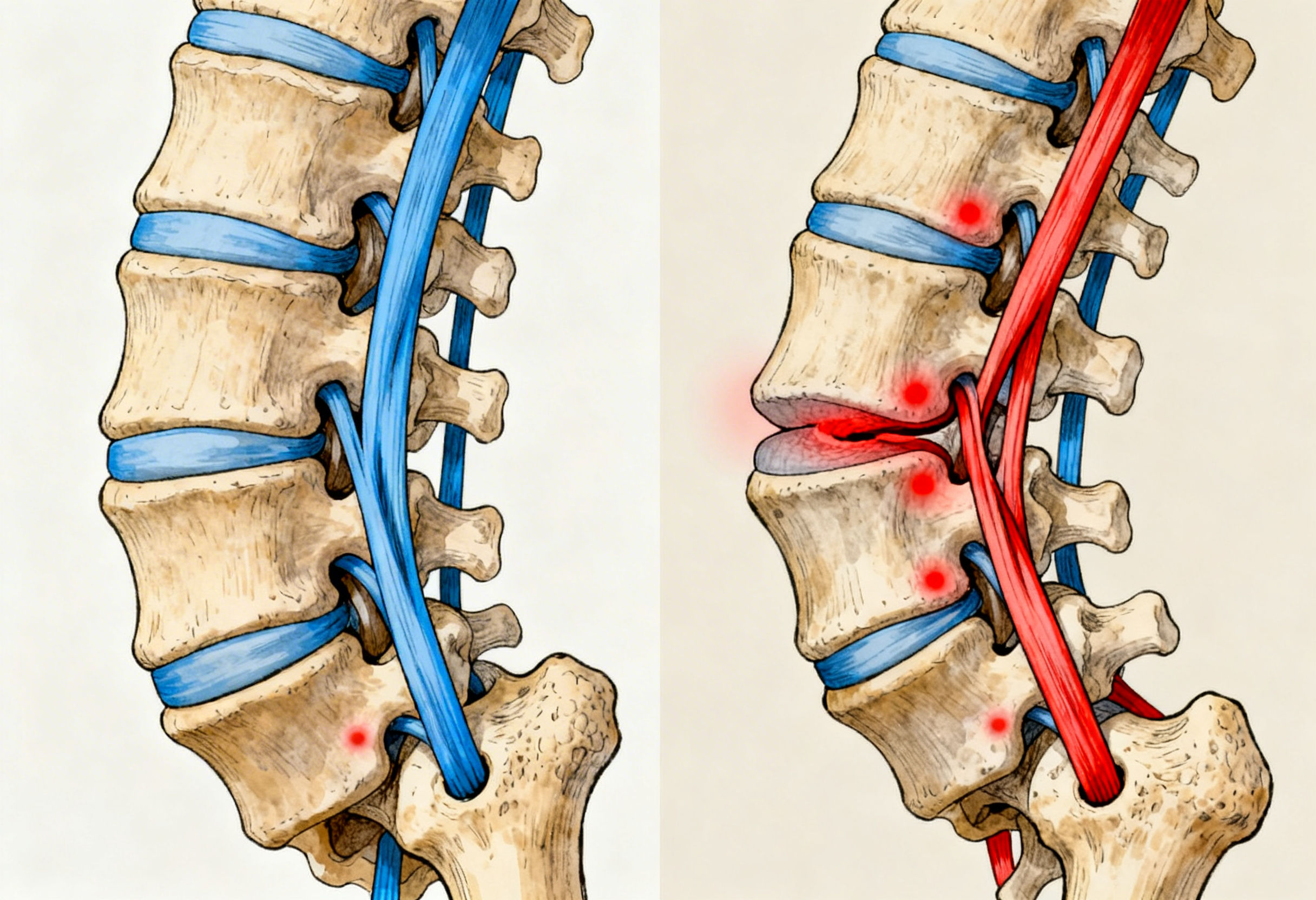
Your spine is built from repeating “modules” called functional spinal units (FSUs): two adjacent vertebrae, the intervertebral disc, facet joints, and a ligament-muscle envelope that controls movement. When movement stays within normal ranges, tissues tolerate load. But when the tension-band system (ligaments and facet capsules) becomes lax, segments can translate or shear more than they should, provoking pain.
Key lumbar stabilizers often implicated in chronic pain patterns:
- Iliolumbar ligament: stabilizes L5 on the sacrum and pelvis, commonly implicated in L5-S1 mechanical stress patterns.
- Sacroiliac ligaments: contribute to SI joint stability; pain can mimic sciatica or gluteal referral patterns.
- Facet joint capsules: guide motion and limit excessive rotation/translation; laxity can provoke facet irritation and arthritic progression.
- Supraspinous/interspinous ligaments: resist excessive flexion; chronic strain can contribute to “catching,” stiffness, and disc stress patterns.
The progression from laxity to degeneration
A common chronic pattern looks like this:
- Microtears and stretch injury in ligament collagen from repetitive load, poor mechanics, or a single event.
- Incomplete healing due to low vascularity of ligament tissue and insufficient remodeling stimulus.
- Segmental instability, causing excessive micro-motion during routine activities.
- Protective muscle spasm (multifidus, erectors, QL) that becomes chronic, painful, and fatiguing.
- Secondary degeneration, including facet overload and compensatory osteophytes; in some cases, narrowing and nerve sensitization.
This model also explains why a patient can have “mild” MRI findings yet severe pain: many pain generators are functional and dynamic, not well-captured on static imaging.
How Dextrose Prolotherapy Works for Lower Back Pain
What is being injected?
In most clinical protocols for low back prolotherapy, the proliferant is hypertonic dextrose (concentrated glucose solution), sometimes combined with local anesthetic and other supportive components based on clinician training and protocol design. Dextrose prolotherapy is widely discussed in the prolotherapy literature and evidence reviews for chronic musculoskeletal pain. (Cochrane)
The mechanism: a controlled healing cascade
Prolotherapy is designed to restart a stalled repair cycle at the ligament-bone interface (fibro-osseous junction) and related supportive tissues.
1) Inflammatory signaling (early phase)
The hypertonic solution creates a localized stimulus that initiates a short, controlled inflammatory response. This is not “bad inflammation.” It is the beginning of a healing program: immune cells arrive, debris is cleared, and repair signaling is turned back on.
2) Proliferation and growth factor signaling
Macrophages and local cells release growth factors that recruit and activate fibroblasts, the collagen-producing cells that build ligament structure.
3) Remodeling and tightening
New collagen is initially laid down in a more immature form, then remodels over weeks to months into stronger, better-aligned collagen that can increase ligament thickness and tension, improving passive stability.
Systematic reviews and clinical series in the prolotherapy literature support the concept of prolotherapy as a regenerative technique used in chronic low back pain populations, though results depend heavily on diagnosis, injection targets, technique, and rehabilitation strategy. (MDPI)
Who Benefits Most: Matching the Therapy to the Pain Pattern
Prolotherapy tends to be most relevant when pain is driven by mechanical instability and ligamentous insufficiency rather than a purely acute inflammatory flare.
Common clinical patterns that raise suspicion of ligament-driven pain
- Pain worsens with prolonged standing, extension, or transitions (sit-to-stand), and improves with bracing or external support.
- Recurrent “episodes” of back giving way or feeling unstable.
- Tenderness over ligament attachment points (iliolumbar, SI ligaments, interspinous ligaments).
- Chronic muscle guarding that returns quickly after massage or dry needling.
- Pain that returns after steroids once the medication effect fades (because stability was never restored).
When prolotherapy may be less central
- Severe neurological deficits, progressive weakness, bowel/bladder red flags, suspected fracture, infection, tumor, or inflammatory spondyloarthropathy need a different pathway first.
- True surgical emergencies or unstable fractures are not prolotherapy cases.
Why Conventional Approaches Often Plateau
1) NSAIDs can reduce symptoms but may not rebuild tissue
NSAIDs can help pain in the short term, but they do not rebuild ligament tension. For patients whose pain is primarily mechanical, symptom control alone often leads to recurrence once normal loading returns.
2) Steroid injections: rapid relief, structural trade-offs
Corticosteroid injections can calm inflammation quickly, but they are not designed to strengthen ligament tissue. Repeated exposure can be problematic for tissue integrity over time in some contexts, which is why regenerative approaches are often explored when the goal is longer-term stabilization rather than short-term suppression.
3) Static imaging can miss instability
MRI and standard X-rays are done at rest. Ligament laxity and micro-motion often require movement-based assessment and high-quality physical examination to identify the true pain driver.
The ARKA Anugraha Hospital Approach: Regeneration Plus Systems Medicine
Prolotherapy is not a standalone “quick fix” at ARKA Anugraha Hospital. Outcomes improve when the body has the resources to build strong collagen and the mechanical environment supports remodeling.
1) Precision assessment before injections
- Functional exam for segmental instability patterns, SI contribution, hip mechanics, gait.
- Targeted imaging review to rule out red flags and clarify anatomy.
- Identifying the true load driver (hip weakness, core timing, foot mechanics, training errors, or occupational load).
2) Metabolic optimization for collagen quality
Chronic high glucose and insulin resistance can worsen collagen quality via glycation and abnormal cross-linking, making connective tissues stiffer and more injury-prone. That is why metabolic markers and nutrition are not “extra” in regenerative care. They are central.
3) Endocrine and recovery inputs
Tissue repair is anabolic. Poor sleep, chronic stress physiology, and low anabolic signaling can blunt healing. ARKA’s integrative model evaluates recovery capacity and addresses it practically: sleep, protein adequacy, micronutrients, and lifestyle levers that directly influence repair biology.
4) Gut-joint axis and systemic inflammatory tone
Low-grade inflammation from gut dysfunction can amplify pain sensitivity and interfere with recovery signaling. Supporting gut integrity and reducing inflammatory burden can improve the “signal-to-noise ratio” for tissue repair.
5) Rehabilitation that matches tissue remodeling
Ligaments remodel according to load. The goal is not rest forever; it is intelligent progressive loading after the appropriate window, so new collagen aligns along functional stress lines.

What the Procedure and Recovery Typically Look Like
During the session
- Cleaning, localization of targets, and injections at selected ligament attachment points and supportive structures.
- Some discomfort is expected because targets can be sensitive.
After the session
- A post-injection “flare” of soreness is common for several days. This is consistent with the intended inflammatory signaling that starts the repair cascade.
- Most patients continue work, with brief activity modifications.
Course of care
- Many protocols use multiple sessions spaced several weeks apart to allow remodeling between treatments. Evidence reviews describe variable protocols across studies, which is one reason outcomes differ across clinics and populations. (MDPI)
Clinical Bottom Line
If your back pain keeps returning despite physiotherapy, medications, or “normal imaging,” it is worth asking a different question: Is my spine mechanically stable, or am I repeatedly loading lax tissues that never fully repaired?
Prolotherapy for lower back pain is a regenerative option that targets the stability deficit directly by stimulating ligament repair. When paired with integrative inputs that improve collagen quality and recovery biology, it can be a meaningful, non-surgical pathway for carefully selected patients. Evidence syntheses continue to evaluate prolotherapy’s role in chronic low back pain, with patient selection and protocol quality being decisive. (MDPI)
FREQUENTLY ASKED QUESTIONS
- What is prolotherapy for lower back pain?
A regenerative injection technique, most commonly using hypertonic dextrose, designed to stimulate ligament repair and improve spinal stability. - Is prolotherapy the same as PRP?
No. PRP uses platelet-derived growth factors from your blood. Prolotherapy uses a proliferant (often dextrose) to trigger a repair cascade. They can be complementary in select cases. - Is prolotherapy painful?
Mild to moderate discomfort can occur during injections. Post-treatment soreness for a few days is common and expected. - How many sessions are usually needed?
Many patients undergo a series of sessions spaced a few weeks apart. The number depends on instability severity, tissue quality, and response. - How soon will I feel results?
Some people notice early improvement, but structural remodeling is gradual. Meaningful stability changes often evolve over weeks to months. - Can I keep working after prolotherapy?
Most people can continue routine work, with short-term modification of heavy lifting or high-impact activity as guided by the clinician. - Should I avoid NSAIDs around treatment?
Often yes, because NSAIDs can blunt the intended inflammatory signaling that initiates repair. Your clinician will advise based on your medical history. - Is prolotherapy safe?
When performed by trained clinicians with proper technique and screening, prolotherapy has a long history of clinical use and is generally well-tolerated. (Cochrane) - Will prolotherapy help a disc bulge?
It does not “shrink a disc” directly. It can help if disc stress and pain are being driven by instability and segmental overload. - What if my MRI is normal?
A normal MRI does not rule out functional instability or ligament pain. Dynamic assessment and clinical examination can be more revealing. - Is prolotherapy a replacement for physiotherapy?
No. It works best with a structured rehab plan that retrains movement, core timing, hip control, and progressive loading. - Can it help SI joint pain?
It may help when SI pain is driven by ligament laxity and instability patterns rather than purely inflammatory disease. - Are results permanent?
If stability improves and loading patterns are corrected, benefits can be long-lasting. New injury or repeated overload can still cause recurrence. - Who should not do prolotherapy?
Patients with red-flag conditions (infection, fracture, tumor, progressive neuro deficits) require different urgent evaluation first. - What makes ARKA’s approach different?
ARKA combines precision regenerative care with systems medicine: metabolic optimization, gut-joint axis support, recovery biology, and targeted rehabilitation.
Explore Arka Recipes
Discover recipes that blend taste with health, crafted by our experts for your well-being.

Arka Diagnostics
Discover groundbreaking diagnostic services exclusive to India, now available at Arka Health, Bangalore